A left-sided gallbladder is a gallbladder located on the left side of the round ligament. It constitutes an uncommon anatomic abnormality. We report on a case of left-sided gallbladder discovered incidentally during laparoscopic cholecystectomy, and we discuss the different forms of this anatomic anomaly and its surgical relevance.
INTRODUCTION
A left-sided gallbladder (LSG) is a gallbladder located on the left side of the round ligament and not on the right side, which is its common location. It constitutes an un- common abnormality first described from Hochstetter in 1856.
The reported incidence of this anomaly is estimated to be between 0.1% and 1.2%.1– 4 The present case report demonstrates a case of LSG identified during laparoscopic cholecystectomy. Herein, we discuss the different forms of LSG and the surgical relevance of this anomaly.
CASE REPORT
A 50-year-old Caucasian male presented to our surgical clinic with a 3-day history of acute epigastric discomfort and vomiting. The clinical examination revealed no pathological signs and no elevated temperature. His blood results showed that white blood cell count, bilirubin, al- kaline phosphatase, alanine transferase, and gamma-glu- taryl transferase were in the normal range.
An abdominal ultrasound was performed, which showed gallstones in the gallbladder, whereas the diameter of the common bile duct (CBD) was normal (3.7 mm), suggest- ing the absence of obstruction and the presence of gall- stones in the CBD. No other pathology was identified, and cholelithiasis was the presumed diagnosis.
The patient was informed of the diagnosis, and a laparo- scopic cholecystectomy was performed. During the proce- dure, after the insertion of the umbilical port (10mm), we incidentally discovered a left-sided gallbladder (LSG) located under the third hepatic segment at the left of the round ligament (Figure 1).
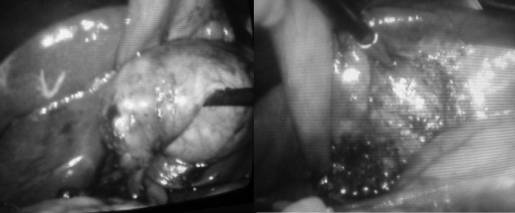
Consequently, the positions of the surgeon and the assistant were modified appropriately to the left side of the patient, and the patient was turned in a left-side up position to optimize the view of the gallbladder and Calot’s triangle. A trocar was inserted in the middle line, middle of the distance between the umbilicus and the xi- phoid (10 mm), and the 2 lateral subcostal ports (5 mm) were placed on the left midclavicular and left anterior axil- lary lines of the abdomen, respectively (Figure 2).

After dissecting Calot’s triangle, we identified the cystic duct, the common hepatic duct junction, and the cystic the gallbladder is located on the left lobe of the liver. In this situation, 2 subtypes can be found according to the way the cystic duct (CD) joins the biliary tree.1 The cystic duct joins the common bile duct (CBD) from the right side as in our case. The explanation of this variation may be that the normal gallbladder bud migrates to the left lobe instead of the right and lies on the left side of the round ligament.2 The cystic duct and the cystic artery, the gallbladder was excised as usual. The patient recovered uneventfully and was discharged on the first postoperative day.
DISCUSSION
Left-sided gallbladder (LSG) without situs inversus can be found in 2 anatomic variants. First is the true LSG, where the gallbladder is located on the left lobe of the liver. In this situation, 2 subtypes can be found according to the way the cystic duct (CD) joins the biliary tree. The cystic duct joins the common bile duct (CBD) from the right side as in our case. The explanation of this variation may be that the normal gallbladder bud migrates to the left lobe instead of the right and lies on the left side of the round ligament. The cystic duct joins the left side either of the (CBD) or of the left hepatic duct (LHD) directly and is accompanied by failure in the development of the normal structure in the right side.
Second, the gallbladder is on the left side of the round ligament but still on the right lobe of the liver, because the round ligament has deviated to the right2–3,5 Of 41 patients with LSG, Nagai et al2 found 20 with the cystic duct joining the CBD from the right side and 11 from the left. In 2 patients, the CBD directly joined the right hepatic duct and in one patient the LHD.
Recent studies suggest that routine ultrasonography in patients with gallstone disease often fail to make the diagnosis of LGB disease in the majority of cases,1 which was also the case in our patient. In another study,6 the diagnosis was made only at the time of surgery, despite repeated radiological investigations.
Knowledge of the location of the gallbladder is of great importance for the surgeon, particularly when cholecys- tectomy or other biliary surgery is to be performed. Be- cause there are many variants not only of the position of the gallbladder but also in the way the cystic duct joins the biliary tree, understanding the individual’s anatomy is crucial to avoid injuries to the bile ducts in these patients. Idu et al1 reported 5 cases of LSG and suggested several modifications of the laparoscopic procedure, such as that the right hand operating ports should be placed on the left of the midline, which was the way we performed the procedure in our patient. Hunter et al7 suggested that the preparation and clipping of the cystic duct should be performed as nearly as possible to the infundibulum, after the surrounding tissue is stripped down.
CONCLUSION
LSG is a rare abnormality in the position of the gallbladder that consists of several subvariations referred to as the cystic duct course. The recognition of them is important when performing cholecystectomy to avoid injury to the biliary tree.
References:
- Idu M, Jakimowicz J, Iuppa A, Cuschieri A. Hepatobiliary anatomy in patients with transposition of the gallbladder: impli- cations for safe laparoscopic cholecystectomy. Br J Surg. 1996; 83:1442–1443.
- Nagai M, Kubota K, Kawasaki S, Takayama T, Bandai Y, Makuuchi M. Are left-sided gallbladders really located on the left side? Ann Surg. 1997;225:274 –280.
- Maetani Y, Itoh K, Kojima N, et al. Portal vein anomaly asso- ciated with deviation of the ligamentum teres to the right and malposition of the gallbladder. Radiology. 1998;207:723–728.
- Hsu SL, Chen TY, Huang TL, et al. Left-sided gallbladder: its clinical significance and imaging presentations. World J Gastro- enterol. 2007;13:6404 – 64049.
- Ozeki Y, Onituka A, Hino A. Anomalous branching of intra- hepatic portal vein associated with anomalous position of round ligament. Kanzou. 1989;30:372–378.
- Wong LS, Rusby J, and Isamil T. Left-sided gallbladder: a diagnostic and surgical challenge. ANZ J Surg. 2001;71:557–558.
- Hunter LG. Exposure, dissection and laser versus electrosur- gery in laparoscopic cholecystectomy. Am J Surg. 1993;165:492–





